U.S. Led in Contributions but Failed to Receive Commensurate Benefits
In the two-year period ending at the close of 2019, the U.S. contributed $893 million to the World Health Organization, according to WHO records. China contributed just under $86,000 during that period according to The Wall Street Journal.
Did the U.S. and the Rest of the World Get the Value Promised by WHO as the Coronavirus Pandemic Swept the Globe?
In light of the pandemic, I examined which nations provide the most funding for the WHO Health Emergencies Programme. Then I evaluated which continent receives the most benefit. I also reviewed the mix between ‘headquarters,’ which is staff and administrative functions vs. people and programs on the ground delivering benefits.
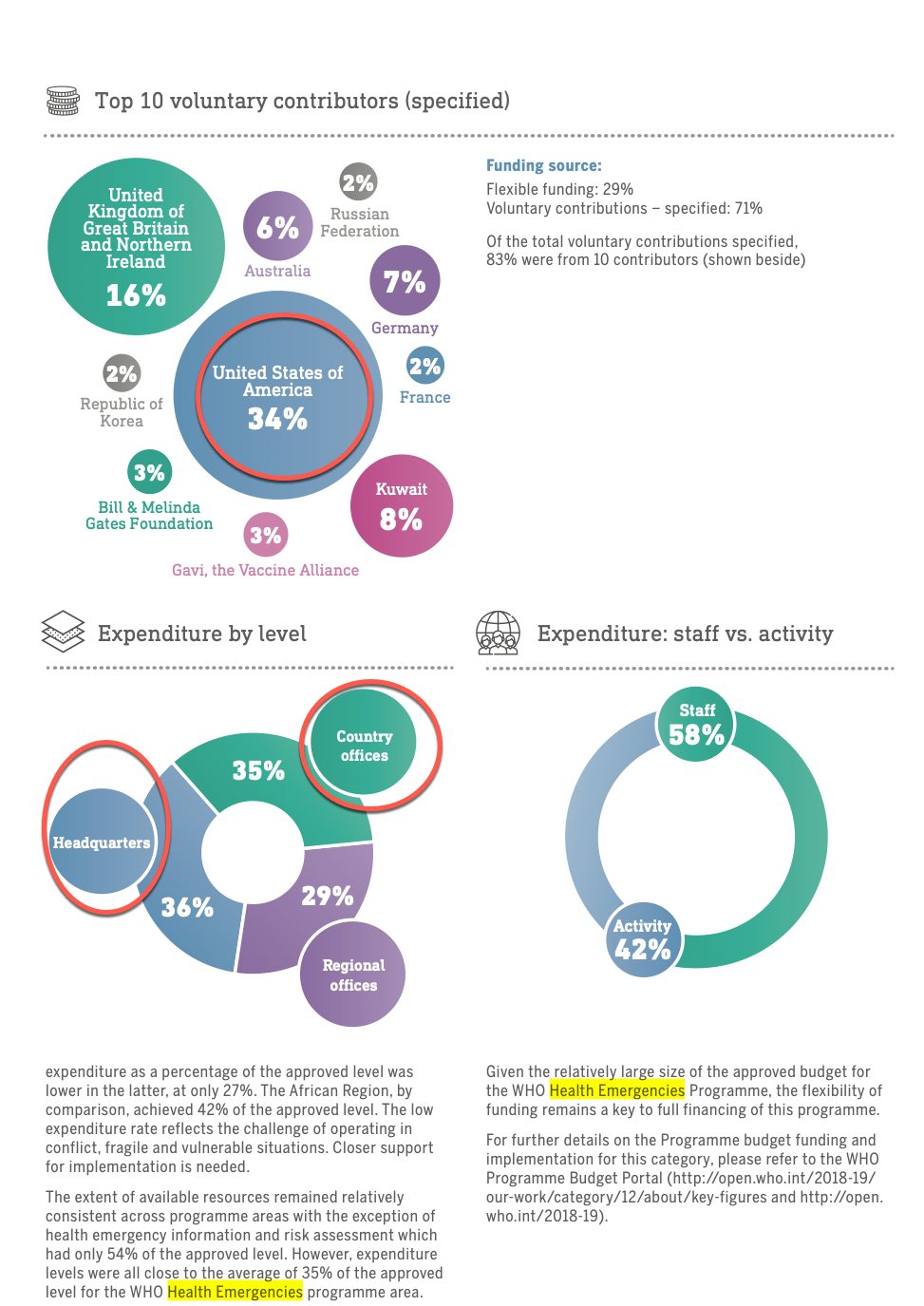
WHO publishes data by “programme,” so this is only a look at the Health Emergencies section. Surprisingly, the World Health Organization spends 58% of its budget on ‘staff’ and 42% on ‘activity.’
Findings
The programme is described as follows:
Rapidly detecting health emergencies – WHO has a system for carrying out continuous event-based surveillance of public health events and verification and assessment of detected events. It currently picks up 7000 public health threat signals every month, of which 0.5% result in formal field investigations and risk assessments.During outbreaks, WHO provides support to countries for continuously monitoring events and conducting risk assessments, including implementation of the Public Health Information System. WHO’s Disease Outbreak News (DONs) provides updates containing epidemiological summaries, responses, risk assessments and advice. DONs are among the most visited WHO webpages, receiving nearly three million visits a year. In 2018, WHO published 91 DONs. The Early Warning, Alert and Response System (EWARS) is a new computer programme developed by WHO for outbreak detection in emergency settings. It allows for quick collection of field data to enable a prompt response.
The United States gives 34% of the budget for the WHO Emergencies Programme, over twice as much as the next country which is the United Kingdom at 16% Yet, the all of the Americas including North and South America receive only 9.6% of the spending, whereas Africa receives nearly 50% of budgeted funds. Perhaps this is because of historical threats from Ebola. Nonetheless, it raises a question of the surveillance methods used to identify and mobilize resources for non-African, non-Ebola emergencies such as coronavirus and the COVID-19 pandemic.
Additionally, WHO touted the following capabilities:
Some flagship networks include:
Global Influenza Surveillance and Response System – a 66-year-old network comprising 150 institutions in 114 countries, it generates data for vaccine composition and offers guidance on influenza pandemic preparedness.
Emerging Diseases Clinical Assessment and Response Network – defines standards of care, such as clinical standards and standard operating procedures, and, in emergencies, deploys clinical experts to the front line.
Emerging and Dangerous Pathogens Laboratory Network – focuses on human and veterinary infections by following an integrated approach to laboratory response.
During the Ebola outbreak, 24 million tests were administered under the auspices of WHO. According to the World Health Organization:
Previously, testing for Ebola virus disease could take days or even a week. A lack of local laboratory capacity meant that samples had to be sent to highly secure laboratories far from the outbreak location. This wasted precious time for the patient and allowed the undetected virus to spread. The arrival of a rapid genetic test for the Zaire strain of Ebola, the Xpert Ebola test, changed that. Developed during the 2014–2016 Ebola virus disease outbreak, the test uses the GeneXpert machine to produce results in under two hours instead of several days, allowing the rapid initiation of patient care and containment measures. The test can be safely implemented in provisional laboratories near patient care settings; it is simpler to use than a conventional polymerase chain reaction, and can be operated by locally-trained staff. During the Ebola virus disease outbreak, new laboratories could be set up in 48 hours to move with the outbreak, and 13 500 GeneXpert samples were tested.
According to Joe Hasell, Esteban Ortiz-Ospina, Edouard Mathieu, Hannah Ritchie, Diana Beltekian and Max Roser who published their findings in Our World Data:
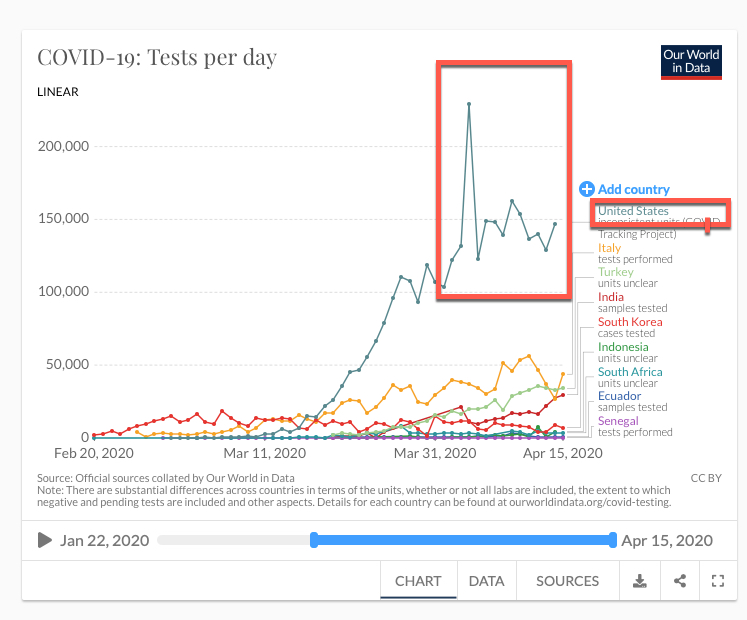
U.S. Leads the World in COVID-19 Testing
“The most common way of performing a test of this type is with a ‘PCR’ test. The main problem is that these tests are not always accurate.
The second kind of test – serological tests – are generally still in the research stage of development. This kind of test will be central to establishing how far the coronavirus has spread across the broader population. The Centre for Health Security at Johns Hopkins University provide up to date information on serology tests that are in development or available for use – whether for diagnosis, or only for research purposes.A helpful summary of the current state of testing technologies and their implementation – as of 8 April – can be found in this editorial published in Nature Biomedical Engineering.
Is WHO Relevant, now that it is Likely that China Caused the Pandemic Executed a Cover-Up?
Where was WHO when we needed them? One thing is clear. No global organization can withstand scrutiny with a spend of 58% on staff and only 42% on programs.
Most of WHO’s opening remarks in the source document for this analysis focus on universal healthcare, not on managing pandemics. Universal healthcare does little to protect us from COVID-19. Currently the U.S. leads the world in the number of tests per day for COVID-19. It’s hard to see how the World Health Organization can take credit for that.
The World Health Organization excerpted charts on donors, staff costs and actual activities are below:
World Health Organization contributors to the WHO Emergencies programmesThe World Health Organization budget for 2018 to 2019 for emergencies
Michael Arrigo, an expert witness, and healthcare executive, brings four decades of experience in the software, financial services, and healthcare industries. In 2000, Mr. Arrigo founded No World Borders, a healthcare data, regulations, and economics firm with clients in the pharmaceutical, medical device, hospital, surgical center, physician group, diagnostic imaging, genetic testing, health I.T., and health insurance markets.
His expertise spans the federal health programs Medicare and Medicaid and private insurance. He advises Medicare Advantage Organizations that provide health insurance under Part C of the Medicare Act. Mr. Arrigo serves as an expert witness regarding medical coding and billing, fraud damages, and electronic health record software for the U.S. Department of Justice. He has valued well over $1 billion in medical billings in personal injury liens, malpractice, and insurance fraud cases.
The U.S. Court of Appeals considered Mr. Arrigo's opinion regarding loss amounts, vacating, and remanding sentencing in a fraud case. Mr. Arrigo provides expertise in the Medicare Secondary Payer Act, Medicare LCDs, anti-trust litigation, medical intellectual property and trade secrets, HIPAA privacy, health care electronic claim data Standards, physician compensation, Anti-Kickback Statute, Stark law, the Affordable Care Act, False Claims Act, and the ARRA HITECH Act.
Arrigo advises investors on merger and acquisition (M&A) diligence in the healthcare industry on transactions cumulatively valued at over $1 billion. Mr. Arrigo spent over ten years in Silicon Valley software firms in roles from Product Manager to CEO. He was product manager for a leading-edge database technology joint venture that became commercialized as Microsoft SQL Server, Vice President of Marketing for a software company when it grew from under $2 million in revenue to a $50 million acquisition by a company now merged into Cincom Systems, hired by private equity investors to serve as Vice President of Marketing for a secure email software company until its acquisition and multi $million investor exit by a company now merged into Axway Software S.A. (Euronext: AXW.PA), and CEO of one of the first cloud-based billing software companies, licensing its technology to Citrix Systems (NASDAQ: CTXS).
Later, before entering the healthcare industry, he joined Fortune 500 company Fidelity National Financial (NYSE: FNF) as a Vice President, overseeing eCommerce solutions for the mortgage banking industry. While serving as a Vice President at Fortune 500 company First American Financial (NYSE: FAF), he oversaw eCommerce and regulatory compliance technology initiatives for the top ten mortgage banks and led the Sarbanes Oxley Act Section 302 internal controls I.T. audit for the company, supporting Section 404 of the Sarbanes Oxley Act. Mr.
Arrigo earned his Bachelor of Science in Business Administration from the University of Southern California. Before that, he studied computer science, statistics, and economics at the University of California, Irvine. His post-graduate studies include biomedical ethics at Harvard Medical School, biomedical informatics at Stanford Medical School, blockchain and crypto-economics at the Massachusetts Institute of Technology, and training as a Certified Professional Medical Auditor (CPMA). Mr. Arrigo is qualified to serve as a director due to his experience in healthcare data, regulations, and economics, his leadership roles in software and financial services public companies, and his healthcare M&A diligence and public company regulatory experience.
Mr. Arrigo is quoted in The Wall Street Journal, Fortune Magazine, Kaiser Health News, Consumer Affairs, National Public Radio (NPR), NBC News Houston, USA Today / Milwaukee Journal Sentinel, Medical Economics, Capitol ForumThe Daily Beast, the Lund Report, Inside Higher Ed, New England Psychologist, and other press and media outlets. He authored a peer-reviewed article regarding clinical documentation quality to support accurate medical coding, billing, and good patient care, published by Healthcare Financial Management Association (HFMA) and published in Healthcare I.T. News.
Mr. Arrigo serves as a member of the board of directors of a publicly traded company in the healthcare and data analytics industry, where his duties include: member, audit committee; chair, compensation committee; member, special committee.